
Aniridia Genetics
Simply put, genes hold the information to build and maintain an individual’s cells. All organisms have many genes corresponding to various biological traits, some of which are immediately visible, such as eye color or hair color.
Minute changes in these genes (mutations) can have big consequences. In the vast majority of cases, aniridia is caused by a mutation in the PAX6 gene located on the short arm of chromosome 11 (11p13). If an individual has a normal PAX6 gene, another gene mutation may be mutated. Possible genes include: PITX, FOXC1, cypB, GDF6, or other. In relation to aniridia, most information and data is known about the PAX6 gene.
Inheritance and the Genetic Types of Aniridia
Every individual has two copies of every gene: one from their father and one from their mother. Unlike most genetic conditions, aniridia is dominant. It only takes one copy of the mutated gene to have the condition. Consequently, if a person with aniridia has a child, there is a 50% chance the child will have aniridia. There are four basic types of aniridia:
1. Familial aniridia (autosomal-dominant) is the most common form of aniridia. Familial aniridia is inherited directly from a parent who has aniridia. In familial aniridia, there is a mutation of the PAX6 gene.
2. Sporadic aniridia is the second most common form of aniridia. In this case, both parents have normal chromosomes and genes. However, in the affected child, a new change (mutation) of the PAX6 gene, whose cause is unknown, occurred before or soon after conception.
3. WAGR syndrome is a very rare form of sporadic aniridia (both parents have normal genes) where there is not only a mutation of the PAX6 gene but also involves a deletion of the neighboring genes on chromosome 11. In addition to the common traits of aniridia, children with WAGR have a high risk for developing Wilms’ timor and other medical complications such as genital abnormalities and learning and behavioral difficulties. Early diagnosis of WAGR is essential for monitoring and treating Wilm’s tumor and other complications.
4. Gillespie syndrome is an extremely rare (there are only a few documented cases) type of aniridia and is not thought to be associated with a PAX6 mutation. This type of aniridia is characterized with a particular appearance of the iris remnant (described as having a “scalloped” border) mental retardation, and cerebellar ataxia, (muscle incoordination).
Genetic Testing for Aniridia
Genetic testing for aniridia can be coordinated through a genetic counselor. Genetic counselors are generally affiliated with universities and/or children’s hospitals.
Aniridia’s Impact on Vision
One of the first things a parent often wonders is ‘What will my child see? What will his acuity be?’ People with aniridia are generally considered to have ‘low vision’ or be ‘visually impaired’ which means their vision reduction cannot be corrected with standard glasses or contact lenses. It is not possible to predict what a child’s vision will be in infancy because it depends on many factors.
In order to understand how the differences in the structure of the eye in an individual with aniridia impacts vision, it’s helpful to have a basic understanding of how vision works. If you need a ‘refresher’, please see the section of our website How Vision Works to understand how the different parts of the anatomy of the eye work together to allow us to perceive light and see.
Although people with aniridia always have vision problems, the degree varies greatly and largely depends on which parts of the anatomy of the eye were affected in the individual. All people with aniridia lack an iris (the term ‘aniridia’ literally means ‘without iris’). In addition, most also have one or more malformations of the eye that impact their vision.
Below is a description of each of the parts of the eye that can be affected by aniridia and the associated impact on vision. We’ve included an overview of some key ocular problems associated with aniridia.
The Iris
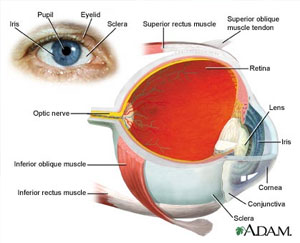
The iris is the colored part of the eye. It helps to control the amount of light entering the eye. The iris works in conjunction with the pupil (the black dot in the middle of the eye) to control how much light enters the eye. The iris has tiny muscles which enable it to dilate and constrict the pupil to allow more or less light into the eye. Simply put, when it is darker, it opens more, to allow more light in so we may see better. When it is bright, it constricts to limit how much light enters the eye through the pupil, so the more delicate parts of the eye are not damaged. Individuals with aniridia are born without or with very minimal iris in both eyes.
Diagnosis: The lack of iris is most likely the primary diagnosis of aniridia and indeed, the most obvious (individuals with anirdia don’t have an eye color, rather, they are all ‘pupil’ or black-eyed). Generally, a pediatric opthalmologist will diagnose aniridia following an exam.
Impact on vision: All individuals with aniridia have little or no iris in either eye (sometimes there is a partial iris). The lack of iris and its impact on vision remains constant throughout an individual’s lifetime. As a result of the lack of iris, individuals with aniridia are often sensitive to bright lights and glare, which is usually helped by wearing sunglasses and/or hats outside and mildly-tinted lenses inside.
In addition, because light is not being filtered, individuals usually experience reduced acuity as a result of light flooding into the back of the eye (if you have ever had your eyes dilated for a vision test, you may notice that vision is a little ‘blurry’. Individuals with aniridia always have dilated eyes.)
Some individuals with aniridia have had success with special contacts with a ‘painted’ iris. However, contact lens use in individuals with aniridia must be closely monitored because contacts can harm the cornea (see below). The type of contact lens and frequency of use is very important.
Another consequence the malformed iris can have is closed-angle glaucoma (see Glaucoma section below).
Current medical/surgical Treatments: The lack of iris can be corrected with an iris implantation surgery, although it is not yet approved by the FDA. Currently, iris implants are only performed in combination with a cataract procedure (see lens section below). An iris implant can help control the amount of light entering the eye. Some individuals with aniridia have been successful with the iris implant operation. Others have had problems associated with the implant, specifically “aniridia fibrosis.” Aniridia fibrosis means a fibrotic tissue forms in the anterior chamber. The hypothesis is that this fibrotic tissue is formed because implanted devices are near or touching immature vessels. Such a condition is NOT always present with implanted devices in patients; however, it certainly should be monitored. Should the fibrosis become present, early surgical intervention is recommended.
The Cornea
The cornea is like the windshield of the eye. A normal, healthy cornea is a clear, avascular (lacking blood vessels) transparent tissue that allows light to pass through. Most individuals with aniridia are born with a clear, healthy cornea. However, unlike the iris, the cornea is one area of the aniridic eye that degrades and causes vision to degenerate over time.
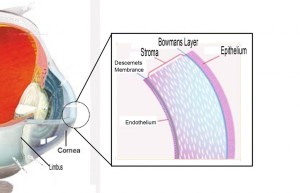
Impact on vision: In order to understand the impact on vision, it is helpful to have a general understanding of the biology of the cornea and the adjacent limbus region:
The limbus (see diagram) is the border of the cornea and the sclera (whites of the eye). The limbus region is responsible for creating stem cells that ‘refresh’ the clear epithelium of the cornea (think of the epithelium as the ‘skin’ on the cornea, much like the skin on our bodies, but this skin is clear, not opaque). In individuals with aniridia, these stem cells do not function properly. For some unknown reason, the mutated PAX 6 gene in people with aniridia disrupts the signal for the cornea to refresh itself. Over time the opaque epithelial cells and vascularization (veins) from the conjunctive begin to grow over the clear cornea and cover the cornea starting from the periphery of the cornea and working its way into the center. The result is that the ‘clear window’ of the cornea changes into the transparency of wax paper.
As the diagram shows, the cornea is made up of 5 layers. Each layer needs to be healthy to maximize vision and keep the other layers intact. Most individuals with aniridia are born with a clear, healthy cornea.
However, by their early teens, the cornea begins to show evidence of the opacification caused by the malfunctioning stem cells. This is called corneal pannus (also called corneal keratopathy or aniridic keratopathy). Corneal pannus is scarring of the corneal tissue. Left untreated, this opacification and vascularization can pass through the epithelial layer (the outermost layer, or the ‘skin’ of the cornea) and cause damage to the stroma layer of the cornea.
The impact on vision of corneal pannus is profound in individuals with aniridia. An individual’s baseline vision is further reduced by having a layer of ‘wax paper’ cover the “windshield”. The result is very little vision.
Current medical/surgical treatments: Treatment of corneal pannus depends on the stage of the disease. In the early stages when the central vision has not yet been affected because the central cornea still has a normal epithelium, the treatment is to keep the surface of the eye as healthy as possible. (Indeed, one way to prolong the health of the aniridic cornea is to keep the surface as healthy as possible by protecting it and making sure it stays lubricated and not dry or inflamed.) However, once the pannus has significantly affected the central vision, the current treatment is surgery.
Because the culprit of the pannus (scarring) is the limbus region (the area generating stem cells to refresh the cornea), this region needs to be addressed with a limbal stem cell transplantation. The most commonly used technique for addressing the malfunctioning limbus region is keratolimbal allograft (KLAL). During the KLAL procedure, limbal tissue from a cadaver or a living-related donor (“allo-” means other) is grafted (“-graft”) onto the aniridic eye. (The scarred tissue is first removed and then the new tissue is grafted). While this procedure has regained sight for thousands of people it has associated risk because of the required systemic immunosuppression drugs (so that the body does not reject the foreign tissue) and if not properly monitored post-surgically, has a high risk of failure. In addition, individuals have a very high incidence of post-surgical glaucoma.
If the scarring has penetrated the stroma layer of the cornea (later stages of the disease), then in addition to the KLAL treatment (or other treatment used to address the limbus region), the individual with aniridia must also have a cornea transplant.
In recent years, some individuals with aniridia have opted for artificial corneas (keratoprosthesis), especially when the individual has had multiple KLAL failures or they cannot tolerate immunosuppression drugs. The benefit to an artificial cornea is that it does not require immunosuppression drugs. However, complications can include glaucoma and retinal detachment. Also, any foreign object in the anridic eye can lead to aniridic fibrosis.
Future treatments or prevention: Hope for the future includes treatments that do not require immunosuppression by using stem cells from an individual’s own body or, even better, preventing corneal keratopathy altogether. The Vision For Tomorrow Foundation is committed to funding research to reach these two goals.
The Lens
The lens is a transparent, biconvex structure in the eye whose function is to focus light onto the macula. Problems that can occur in the lens include cataracts (clouding of the lens), microphakia (abnormal smallness of the lens), and lens subluxation (displaced or malpositioned lens).
Impact on vision: Some individuals with aniridia are born with small cataracts, which are little “dots” clouding the lens. Typically, these small dots do not impact one’s vision. However, as the aniridic eye becomes more affected by the other associated eye problems, such as glaucoma, cataracts can grow and begin to impact vision. Cataracts typically grow very slowly. Cataracts and lens subluxation typically cause a high degree of astigmatism (vision is blurred due to the inability of the optics of the eye to focus a point object into a sharp focused image on the retina). Astigmatism can be helped using properly-prescribed refractive glasses.
Current medical/surgical treatments: In the early stages of cataracts when vision is not significantly impacted, the use of corrective glasses or contact lenses can improve vision. However, contact lens use in individuals with aniridia must be closely monitored because contacts can harm the cornea (see above). The type of contact lens and frequency of use is very important.
Once vision is significantly impacted, cataract extraction surgery may be necessary. An intra-ocular lens may be implanted but carries the risk of aniridic fibrosis.
The Retina
The fovea is the center of the macula – the area of the retina responsible for our central, sharpest vision. In a normal eye, the macula is the area of a person’s best vision that focuses on an image such as a person’s face. The fovea zeros in on detail such as seeing a freckle on someone’s face. In people with aniridia, the fovea is underdeveloped. This is known as foveal hypoplasia. Typically, most individuals with aniridia have foveal hypoplasia to some degree. Foveal hypoplasia is non-degenerative (an individual’s baseline vision does not degenerate due to foveal hypoplasia).
Impact on vision: Because the fovea is responsible for detail vision, the impact on vision is that objects lack detail. Primarily due to the differences in the fovea, individuals with aniridia have a reduced visual acuity. Visual acuity refers to the ability to see fine detail. A good analogy is to think of low- vs. high-resolution pictures. The higher the resolution on a photograph, the clearer or crisper the image. An individual’s “resolution” depends on the degree of foveal hypoplasia. An individual’s visual acuity is an indication of the clarity or clearness of what they are seeing. Visual acuity is typically measured by reading letters on an eye chart. The measurement given is based on what a ‘normal’ human being should be able to see when standing 20 feet away from the eye chart.
If an individual has 20/20 vision, it means that when he stands 20 feet away from the chart, he can see what a “normally-sighted” individual can see at 20 feet away. (In the metric system, the standard is 6 meters and it’s called 6/6 vision.) In other words, if an individual has 20/20 vision, his vision is ‘normal’ – a majority of people in the population can see what he can see at 20 feet. If an individual has 20/100 vision, it means that when he stands 20 feet away from the chart he can only see what a ‘normally-sighted’ person can see when standing 100 feet from the chart. The best-corrected visual acuity for most people with aniridia can vary between 20/40 and 20/400. In general, an individual with aniridia, even after their vision is ‘corrected’ with glasses or lenses to correct lens or cornea refractive abnormalities, must be much closer to the chart to see the same lines than a ‘normally-sighted’ person. Best-corrected visual acuity is the measure of best acuity while wearing corrective lenses like glasses or contact lenses.
A secondary condition thought to be caused by foveal hypoplasia in those with aniridia is nystagmus. Please see the section below for information on nystagmus.
Current medical/surgical treatments: There are no current treatments for fovea hypoplasia. In fact, researchers are continuing to study how the fovea is formed.
The Optic Nerve
The optic nerve is the connection from the eye to the brain. In some people with aniridia, optic nerve hypoplasia, where the nerve is smaller and underdeveloped, is present. Fortunately, this is not common in aniridia. Rather, the optic nerve is more commonly affected by the development of glaucoma (see below).
Glaucoma
Glaucoma is a group of eye diseases that gradually steal sight by harming the optic nerve. In the early stages of the disease, there may be no symptoms. In most cases, glaucoma is caused by increased pressure within the eye. This elevated pressure is caused by a backup of fluid in the eye. Over time, it causes damage to the optic nerve.
In order to best understand what happens in glaucoma, think of the eye as a sink, in which the faucet is always running and the drain is always open. The aqueous humor (the fluid) is constantly circulating through the anterior chamber. This fluid is produced by a tiny gland, called the ciliary body, situated behind the iris. It flows between the iris and the lens and, after nourishing the cornea and lens, flows out through a very tiny spongy tissue, only one-fiftieth of an inch wide, called the trabecular meshwork, which serves as the drain of the eye. The trabecular meshwork is situated at the angle where the iris and cornea meet. When this drain becomes clogged, aqueous can not leave the eye as fast as it is produced, causing the fluid to back up. However, because the eye is a closed compartment, the “sink” does not overflow; instead, the backed-up fluid causes increased pressure to build up within the eye.
To understand how this increased pressure affects the eye, think of your eye as a balloon. When too much air is blown into the balloon, the pressure builds, causing the balloon to pop. Because the eye is too strong to pop, it gives at the weakest point, which is the site in the sclera where the optic nerve leaves the eye. The optic nerve is the part of the eye which carries visual information to the brain. It is made up of over one million very thin nerve cells. When the pressure in the eye builds, the nerve cells become compressed, causing them to become damaged and, eventually, die. The death of these cells results in permanent visual loss.
Impact on vision: Of all the secondary conditions present in individuals with aniridia, glaucoma has the most serious risk of permanently deteriorating vision. Early diagnosis and treatment of glaucoma is crucial to prevent glaucoma from permanently reducing vision. Because individuals with aniridia are at a high risk for developing glaucoma, it is vital that the pressure within the eye be closely monitored.
There are many options for monitoring eye pressure and it is important this be done at every ophthalmology appointment – including the very first one. Typically, a pressure reading for a child should be in the mid- to low-teens. A reading of greater than 20 could mean that glaucoma is present and a glaucoma specialist should be consulted. Pressures can be checked in a few ways. Pressures readings can be performed in the ophthalmologist’s office. Typically, a Tonopen is used to measure the pressure, although there are other instruments that can be used. One such instrument is the iCare Tonometer which has greatly simplified the pressure reading process and comfort level for patients. For some small children with aniridia, sedation may be necessary and the exam may be performed in the operating room. Such a procedure is called an Examine Under Anesthesia or “EUA.”
Current Medical/Surgical Treatments: Increased eye pressures in glaucoma can be managed by eye drops and surgeries. There are many types of eye drops on the market to help lower eye pressure. There also are many surgical options including a trabeculectomy, trabeculotomy, laser surgery, and shunt implantations. A trabeculectomy is a surgical procedure in which the trabecular meshwork is opened up, allowing the aqueous humor to drain more easily. This operation can be performed several times in different areas of the meshwork. A trabeculotomy is a more invasive procedure in which a new drainage angle is made to allow the aqueous humor to drain more effectively. Although this is an outpatient surgery, the eye must be monitored by the surgeon on a daily basis for at least two weeks. Another surgical option is laser surgery, where a laser is used to destroy the ciliary body, which produces the aqueous humor. This slows down the inflow of the fluid thereby reducing eye pressure. When these measures fail, a glaucoma surgeon can surgically insert a shunt (there are several different kinds) which is implanted into the front (anterior) chamber. Because aniridics have a risk for aniridia fibrosis, any implantation procedure should be carefully monitored.
Nystagmus
This disorder is characterized by an irregular, side-to-side involuntary eye movement that may be side-to-side, up and down, or rotary. In individuals with aniridia, nystagmus is thought to be secondary to the foveal hypoplasia. Nystagmus does not go away or disappear but it usually becomes less noticeable with age. Conversely, the eye movements usually become more noticeable if an individual is tired, nervous, or stressed.
Impact on vision: Although individuals with nystagmus do not sense that their eyes are moving, this disorder does make it even more difficult to focus on visual details.
Current Medical/Surgical Treatments: There is a procedure, known as a tenotomy, that, although in early stages, has shown some promise in improving nystagmus. However, there is not much research available for this treatment in people with aniridia. For more information on nystagmus, there is a book called ‘Navigating Nystagmus with Your Doctor’ by Edie Glaser. In addition, there is wonderful online support group, American Nystagmus Network, that is very helpful.
Strabismus
Strabismus is a muscle imbalance of the eye which leads to crossing of the eyes or a “lazy eye.” In esotropia, the eye turns inward. In exotropia, the eye turns outward.
Impact on vision: If uncorrected, strabismus can lead to amblyopia, or the loss of some vision function in the weaker eye.
Current medical/surgical treatments: Strabismus is correctable with glasses, eye-patches and/or surgery.
In the past decade, many surgical advances were made in the field of ophthalmology and some of these surgical treatments were attempted on individuals with aniridia. As we continue to study aniridia, we are learning the aniridic eye is very delicate and any intraocular surgery is risky because of the impact on the other structures of the eye. Many times, a treatment to address one issue can result in another issue (for example, corneal surgery that fixes the cornea but results in glaucoma. Or, glaucoma surgery that results in damage to the limbus region or a cataract.) Also, a condition called aniridia fibrosis, where fibrotic tissue begins to invade the interior of the eye, can deteriorate vision.
A note to the reader: The purpose of this content is to describe the ophthalmic complications related to aniridia, how these complications affect vision, how they are diagnosed and the associated treatments currently available. Whenever possible, this content is written in laymen’s terms. This content is not meant for medical professionals or for a person with aniridia who is trying to decipher which treatment is best for them. Rather, this content is meant to provide the reader (most likely a parent or individual with aniridia) with a better understanding of aniridia. Aniridia affects individuals very differently and the reader should always rely on his or her medical doctor when diagnosing and treating any condition.